This Printable Business Form Template belongs to these categories: medical
Subscribe to my free weekly newsletter — you'll be the first to know when I add new printable documents and templates to the FreePrintable.net network of sites.
123 Main St., Apt. #5
Anytown, CA 95928
(555) 555-1212 [email protected]
November 8, 2008
Anytown Medical Center
345 Goodhealth Place
Anytown, CA 95928
To Whom It May Concern:
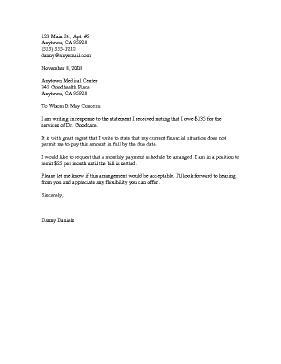
I am writing in response to the statement I received noting that I owe $135 for the services of Dr. Goodcare.
It is with great regret that I write to state that my current financial situation does not permit me to pay this amount in full by the due date.
I would like to request that a monthly payment schedule be arranged. I am in a position to remit $25 per month until the bill is settled.
Please let me know if this arrangement would be acceptable. I'll look forward to hearing from you and appreciate any flexibility you can offer.
Sincerely,
Danny Daniels
People who printed this business form template also printed...
DISCLAIMER: The business forms and letters contained on BusinessFormTemplate.com are not to be considered as legal advice. All content is for informational purposes, and Savetz Publishing makes no claim as to accuracy, legality or suitability. The site owner shall not be held liable for any errors, omissions or for damages of any kind.
Subscribe to the Free Printable newsletter. (No spam, ever!)
This Printable Business Form Template is available to download for free, or you can download the entire collection for only $199.
The free version is available in your choice of DOC or PDF formats. The DOC version can be opened, edited, and printed using Word, Google Docs, etc. The PDF version can be opened and printed with any PDF viewer.
The $199 version includes all of the Printable Business Form Templates on this site, in DOC and PDF formats. After purchase, you can download them and use just a few business forms or the entire collection.