Use this report for employees to fill in when they have been injured while on the job.

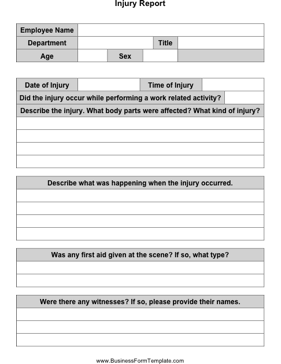
Injury Report
Fields: employee name, department, title, age, sex, date of injury, time of injury
Did the injury occur while performing a work related activity?
Describe the injury. What body parts were affected? What kind of injury?
Describe what was happening when the injury occurred.
Was any first aid given at the scene? If so, what type?
Were there any witnesses? If so, please provide their names.
If patient was transported to hospital or clinic, give the info:
Name of hospital or clinic:
Describe the treatment provided.
Did the employee miss any work?
Additional Notes:
Date:_________ Employee Signature: ___________________________